One of our clients was found murdered today, by the by. Found down by the riverbank, no-one arrested as yet. A mood of mild despondency pervades Central.
Anyway.
One of those originless science facts people quote at you says you are probably sitting no more than six feet from a spider. Proponents of this argument point to the sheer number of the little bastards - hundreds per square metre in normal temperate environment. So, where-ever you are, whatever you are doing, take two paces and there's a spider.
And what brings this to mind?
Well, yesterday I was speaking to a doomed woman. She came in to see me at Southern, her three monthly appointment to see how things were going on the methadone programme.
Our side of things was going well - heroin once, maybe twice in the last year, more out of habit than compulsion, down from four times a day. Got her son back from the welfare, sorted things out with her family. From that point of view things were good.
But elsewhere things were a bit sharp, elsewhere the cracks were beginning to show. Steve - off again, on again partner, in again, out again prisoner - was back inside, and that was both good and bad. Good in that he hit her less. Bad in that her brother hit her more.
There was a pause.
"Your brother" I said. The notes said he was fourteen.
"It's okay" she said. "He's moved out with his girlfriend. I said he couldn't keep bringing his mates around and he went psycho - threw the tv through the window, trashed the house. So I called the cops - he fucked off before they came. Last time it took six of them - and he's ninety five kilos now. He's still under a suspended."
"So he's moved out?"
She nodded. "He did three months in Mauro before. Charged with attempted murder when he was twelve. Stabbed some kid in the chest."
I nodded slowly, in that way you do when you don't want to scream "Oh my God!".
"Just like his fucking father" she said. "But I told them. I'm not putting up with it from Steve and I'm not putting up with it from you. Not with my kid in the house."
"It's good you stood up to it" I said.
"I had to" she said. "Mum's getting out soon, and she needs some place to live. And the thing is, I don't want Joey seeing it. He's only five, but he picks up stuff. And he's big too. Five years old, thirty eight kilos. Can't go to playgroup anymore, got expelled, too violent. All the other kids are terrified of him."
I had this sudden, sharp image of this woman, surrounded by vast, violent men.
Anyway. Soon after that she had to go - and that was the day the first four people who talked to me left my office in tears - and I sat there and tried to remember the exact word from my genetics lectures, fifteen years ago.
Prepotency. That was it. The condition of transmitting "more than your share" of inherited characteristics to your child. Menfolk, if all your children look like your partner, and none look like you, one of the more charitable explanations is that she is prepotent.
Somewhere in that line was a prepotent male, transmitting the genes for violence, large size, maybe the same dark, almost black eyes Joey had (and he was a big kid). And maybe a complementary strand, running through the female line, women who choose men like that.
These are ugly, disquieting thoughts.
Anyhow, I mentioned these to Central's resident psychiatrist the other day, a truly excellent practitioner, and he nodded. He described a child he had seen back in the dark days when he did child psychiatry. The mother had brought the boy to him because he was naughty.
Naughty, in this case, meant torturing animals, smearing faeces on the walls and getting up at night, going into the kitchen, using the gas stove to light a rolled up newspaper and running through the house with it, setting the curtains alight.
"What did you do?" I said.
"What can you do?" said Dr Praecox. "Zonk him out for a few hours every night? Nothing works. And she wouldn't be in it. I think they got some kind of alarm system that went off every time he went into the kitchen."
Anyway - the point I was trying to make is the old one about contours. Look at a contour map.
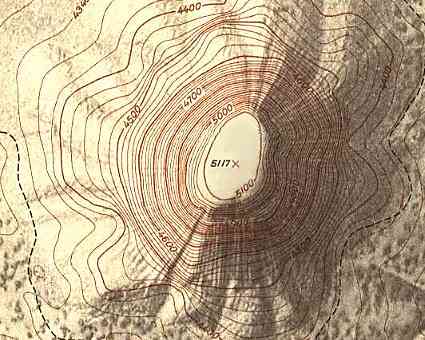
Every closed curve encloses land at a different height - the innermost, land at 5100 whatevers, the next bold one outward 5000, and so on.
It is my suspicion that a similar map can be drawn for the human population.
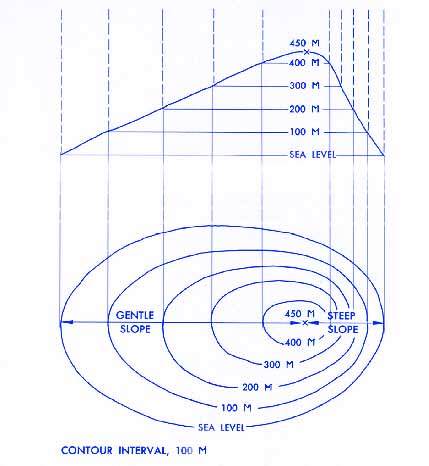
Imagine that on this map -
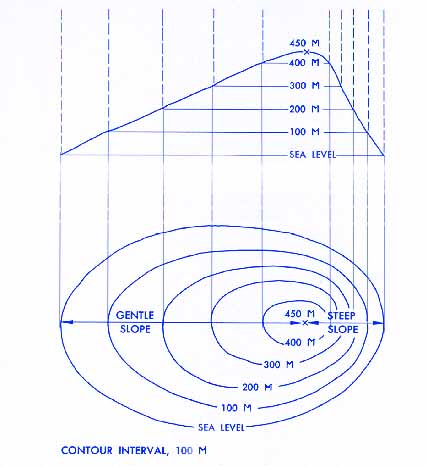
the contour lines do not refer to heights above ground, but rather degrees of madness.
See how every peak is surrounded by an area of ground that is not quite so high. The total area above, say, four hundred metres is smaller than the total area above three hundred metres, and so on.
Well, it's the same with schizophrenia, or bipolar, or antisocial. If pure, classical "DSM IV stamp of approval" schizophrenia, say, is 450 m above sane level, then there is a sizeable group of people around them who fit some, but not all of the criteria. Who, if the peak is depression, have fewer than five of the nine required symptoms - only four. Further down are those who have only three, or have them only some of the time, and so on.
What this means is that there's a sizeable group of people out there with at least one or two signs of mental illness.
Paranoia.
Thoughts of suicide.
Anhedonia.
Compulsive rituals.
That kind of thing.
And of course, life events, especial stressors, psychoactive drugs, these all work like seismic shifts, move us up and down the madness map. It may be that most of the madness map is well above sane level, that there is precious little ground actually
at sea/sane level, that I and everyone whom I have detained or injected with psychoactive drugs is actively part of a majority.
Anyway.
I started thinking about this when Dr Praecox said if we were all only six feet away from a spider, then how far were we away from a psychopath? If we mean someone who stabs kids in the chest at twelve, runs though the house with a burning brand at eight, I hope and pray and suspect we are quite far. But from someone who, caught at the wrong moment? Someone who could, given the right pressures, slip a few metres uphill?
I don't know. The antisocial personality disorder runs at about 2% of the population (3% of men, 1% of women). I don't know what proportion of anti-social PDs are the actual psychopaths, and I know they are not evenly distributed, because many (but I doubt most) of them are in prison. I don't know the maths, but say in a crowd of a thousand, would there be one? And a crowd of a thousand - a few hundred feet from side to side, loosely packed, like at the football or a shopping centre? Or at their homes, a family of two to four per house? Clustered in some families, like the woman who saw me in Southern, little glittering mother lodes of madness.
Too many variables. In the end we guessed at a generous ten kilometres. Big distances out here in the south, semi rural in some places.
You're never more than ten kilometres from a psychopath.
Less morbid posts will return soon.
Thanks for listening,
John




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}